A team of Malaysian cardiologists led by Datuk Dr Tamil Selvan Muthusamy is pioneering a new approach to treating one of the most challenging complications in interventional cardiology: severely hardened and calcified coronary arteries. The research, which began last year, represents a significant step forward in managing patients whose arteries have become so stiffened by calcium deposits that conventional treatment methods struggle to succeed. For the region's healthcare providers and patients facing coronary artery disease, this development carries particular promise as the condition remains a leading cause of mortality across Southeast Asia.
Coronary atherosclerosis develops gradually over years as plaque—a complex mixture of fatty substances, cholesterol deposits, calcium, cellular debris, and fibrin, a blood clotting protein—accumulates along artery walls. Over time, this buildup narrows the vessels, restricting blood flow to the heart muscle. In severe cases, blockages can trigger life-threatening events including myocardial infarction, acute heart failure, or cerebrovascular accidents. For many patients, the standard toolkit of interventional techniques proves sufficient. Procedures such as percutaneous coronary intervention (PCI), coronary artery bypass grafting (CABG), and angioplasty can restore adequate blood flow by widening narrowed passages and stabilising the vessel with stents.
However, when calcium deposits harden excessively within arterial plaque, conventional approaches encounter substantial technical obstacles. As Dr Tamil Selvan explains, the traditional balloon angioplasty method works well for softer plaque. Physicians inflate a balloon to compress the soft material, creating a proper hollow space for blood flow, then deploy a stent to maintain that opening and prevent restenosis—the problematic renarrowing that can occur months or years later. Severely calcified blockages, however, resist this straightforward mechanical compression. The rigidity of calcium-laden plaque demands more aggressive interventions, including rotational atherectomy, high-pressure balloon angioplasty, and intravascular lithotripsy (IVL).
Traditional IVL represents a genuine innovation in this context. This minimally invasive catheter-based system generates ultrasound pulses that create acoustic pressure waves, which in turn fracture calcium deposits within arterial plaque. Yet this breakthrough technology carries practical limitations that constrain its effectiveness in certain clinical scenarios. The device operates on a fixed pulse protocol—older versions deliver eight ultrasonic pulses, newer iterations twelve—requiring physicians to completely fracture calcium deposits within that finite number of pulses. Should the calcification prove more extensive than anticipated, the procedure reaches its technical ceiling. Additionally, the catheter design is comparatively bulky, creating challenges when delivering the device through severely narrowed vessels. The one-size-fits-all balloon dimensions compound these difficulties, since coronary arteries taper irregularly; a single balloon diameter may be appropriate at the vessel's proximal end but prove mismatched further downstream.
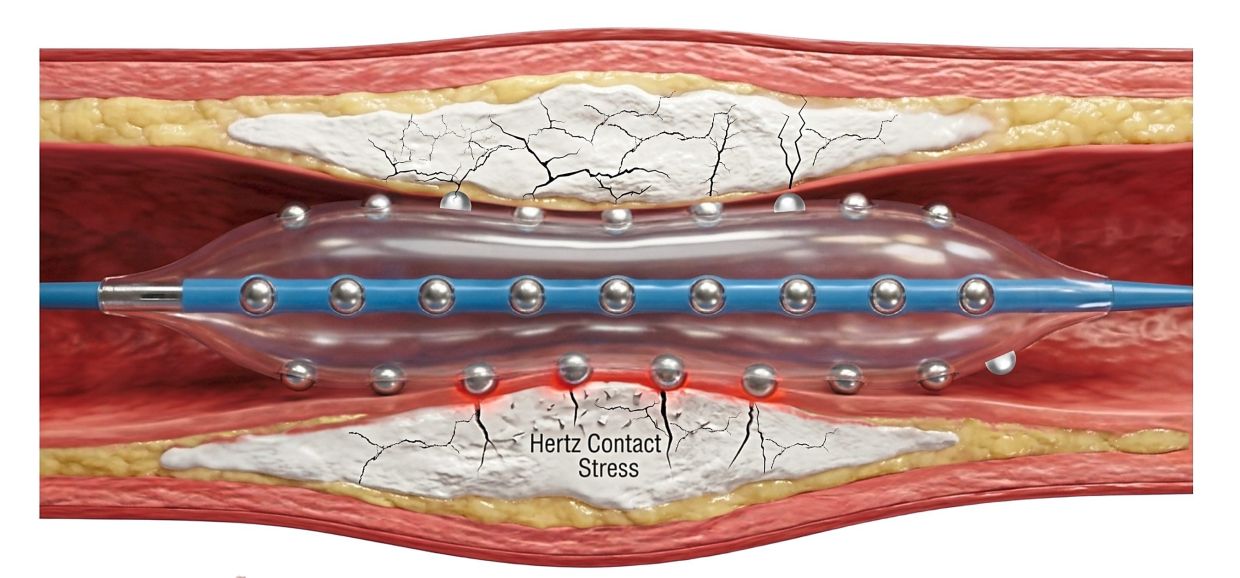
The Hertz Contact-IVL System (HC-IVL), the device now under investigation by Dr Tamil Selvan's team, represents a conceptual departure from energy-dependent lithotripsy. Rather than relying upon an external ultrasound generator, HC-IVL employs a mechanical approach centred on integrated metallic hemispheres embedded within an expandable balloon. When the balloon contacts the hardened plaque surface and pressure is applied, these hemispheric structures create focal pressure amplification—essentially concentrating mechanical force at specific points to crack the calcium. This design yields several clinical advantages. The device generates deep, wide fractures in the plaque without damaging surrounding arterial tissue, allowing the vessel to expand adequately for proper stent deployment. The improved deliverability arises from the catheter's lower profile, permitting it to traverse severely compromised vessels that might reject conventional devices.
Crucially, the mechanical pressure-based design eliminates the pulse-count limitation inherent in energy-based systems. As Dr Tamil Selvan notes, physicians need not complete calcification fracture within a predetermined number of interventions. Moreover, the system's flexibility permits treatment of lengthy lesions or multiple blockages within the same vessel using a single balloon configuration, significantly streamlining complex procedures. For Malaysian patients and those throughout Southeast Asia with advanced coronary calcification—increasingly common as populations age and metabolic disease prevalence climbs—such practical improvements translate into shorter procedure times, reduced radiation exposure during fluoroscopic guidance, and potentially superior long-term outcomes.
Dr Tamil Selvan and his colleagues recognised that while the device's developer had conducted initial safety investigations through small, multi-centre studies in the United States, the evidence base remained limited. Rather than simply adopt an insufficiently validated technology, the Malaysian team determined to undertake a more comprehensive local investigation. This decision reflects responsible clinical stewardship, particularly important given the region's evolving healthcare infrastructure and the critical importance of gathering outcomes data relevant to Asian patient populations, who may differ in genetic predisposition to vascular calcification, metabolic profiles, and comorbidity patterns compared with cohorts in Western clinical trials.
The study design prioritises rigorous safety profiling alongside efficacy assessment. By establishing a well-structured research programme in Malaysia, Dr Tamil Selvan's group contributes to the growing body of evidence supporting this novel technology while simultaneously generating clinical experience that will inform local adoption and training protocols. For Malaysian interventional cardiologists and cardiac surgeons, access to such cutting-edge solutions—coupled with locally derived evidence supporting their use—strengthens the country's position as a regional hub for advanced cardiac care. Hospitals and cardiac centres across Malaysia and neighbouring countries increasingly serve international patients seeking complex interventional procedures, and availability of innovative, well-validated technologies enhances competitive positioning and clinical outcomes.
The research also underscores Malaysia's capacity to drive medical innovation beyond being merely a recipient of imported technologies. As the country continues developing its biomedical sector and research infrastructure, cardiologist-led clinical investigations into novel devices demonstrate the potential for local healthcare professionals to shape global practice standards. For patients throughout Southeast Asia burdened by coronary artery calcification—a condition particularly prevalent in populations with chronic kidney disease, diabetes, and advanced age—successful validation of HC-IVL could substantially expand treatment options and improve survival rates.
The broader context of this research extends to regional health policy considerations. Severe coronary artery disease with extensive calcification imposes enormous economic and social burdens. Myocardial infarction and related complications consume healthcare resources, disable working-age adults, and devastate families. More effective interventional strategies that reduce procedure complexity, hospitalisation duration, and major adverse cardiac event rates yield measurable benefits across public health systems strained by rising cardiovascular disease burden. As evidence from Dr Tamil Selvan's investigation accumulates, healthcare administrators, cardiologists, and policymakers throughout Malaysia and the region will assess how HC-IVL might be integrated into treatment algorithms and reimbursement frameworks.
Looking forward, successful completion of this research programme may establish Malaysia as a centre of excellence for advanced coronary intervention. The country's combination of experienced interventional cardiologists, modern hospital facilities, and growing clinical research infrastructure positions it well to lead investigations into emerging cardiovascular technologies. For the broader Southeast Asian medical community, such leadership generates opportunities for knowledge transfer, training partnerships, and collaborative research that collectively advance the region's cardiac care capability. As cardiovascular disease remains the leading cause of mortality in Malaysia and throughout the region, innovations that extend the boundaries of interventional capability and improve outcomes for the most challenging cases represent investments in population health with profound implications for years to come.

